


Pregnancy and physical activity
Alex Morgan, USA soccer super star, heavily pregnant and still at training, only months before she was supposed to go to the Tokyo Olympics. How do pregnant women deal with physical activity? What is a good amount of activity and when is it too much? What should be encouraged during pregnancy and post partum? What should be watched for or avoided? Where does musculoskeletal physiotherapy play a part?
Since 2016 servicewomen have been fully integrated into the British Armed Forces, including combat roles. However, during pregnancy these duties are downgraded, but can return to full physical and mentally challenging duties, 2 weeks post partum. Little is known about pregnancy and post partum fitness in physically arduous activities. Despite evidence to suggest that women are at risk to pelvic floor dysfunction and musculoskeletal injury, there are no data, nor clinical guidelines on the most appropriate management. Excessive physical activity during pregnancy has been associated with adverse outcomes, including premature delivery, low birth weight, small for gestational weight and preeclampsia. Generally, women reduce their training volume each trimester, whilst no women participate in high impact intense activities in the final trimester. Moreover, the changes induced by pregnancy can last 12 months post partum. Yet, generally, women return to physical activity 6- 12 weeks post partum. Consequently, early return to arduous activities mean that they risk musculoskeletal injury due to deconditioning, potential mental health issues, such as depression, as well as those from the hormonal changes induced ligamentous laxity, altered pelvic floor function, rectus abdominis diastasis and continued changes to hip and back muscular synergies from enhanced anterior pelvic tilt during pregnancy, continuing post partum. Normal timeframes for soft tissue inflammation, proliferation and healing are 12 weeks. Optimal endurance outcome is 16 weeks. Improved strength, at 6-12 weeks, can mask the lack of endurance stability, which requires a longer timeframe for metabolic and mechanical adaptations to take effect. Additionally, people fall roughly into two musculoskeletal categories, the 'floppies' and the 'stiffies'. The former are more adapt to ballistic type of movement activity, whereas the latter more to endurance. This distinction can become clinically important if dealing with synergistic muscular endurance stability post partum. A complete discussion on functional musculoskeletal stability can be read elsewhere on this site : https://www.back-in-business-physiotherapy.com/stability.html
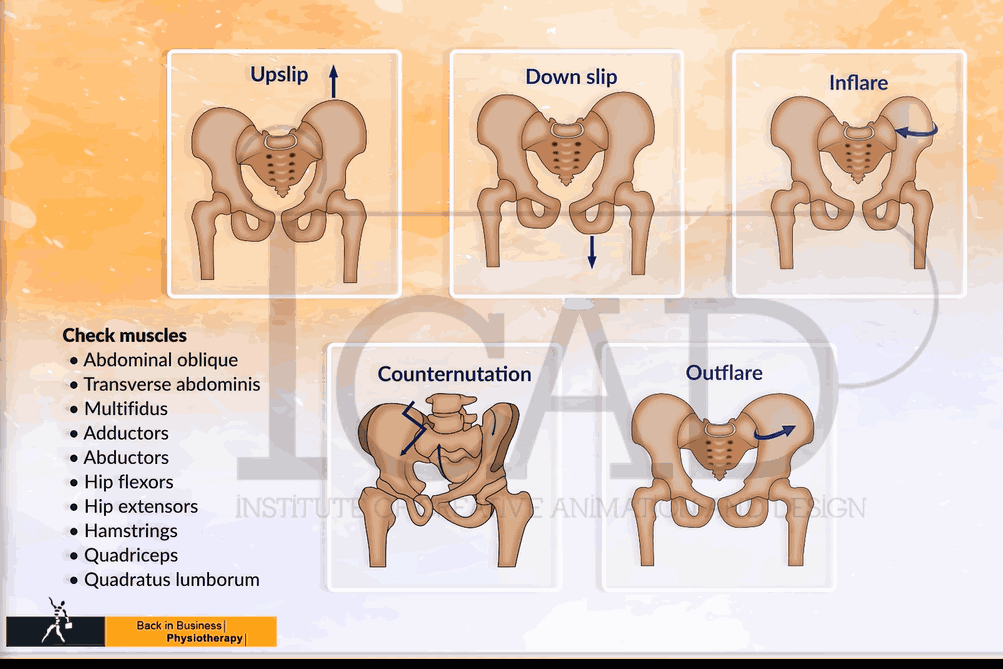
During pregnancy and immediately post partum women experience a number of hormonal and physical changes which can affect their physical and mental capacity to carry out arduous activity. These changes include Estrogen, Oxitocin, Progesterone, Human Gonadotropic Hormone, Prolactin and Relaxin hormones. Physically, the pelvis takes on a more anterior tilt, the sacroiliac joints become more mobile, the pubic symphasis load increases, the lumbar spine increases it's lordosis, superior elevation of the diaphragm with increased expansion is accompanied with increased tensioning of the abdominal muscles and consequential reductions in thoracic rotation. Stride length reduces and a perceived 'waddle' may ensue. Hormonal changes have been studied extensively in women participating in soccer. Interestingly perceived respiratory effort reduces, suggesting care must be taken when using RPE during exercise prescription. Furthermore, pregnancy can induce increases in blood pressure. In other circumstances, breathing exercises have been used to reduce blood pressure and may be considered clinically. Moreover, the sling of muscles crossing the thoracic-lumbar-pelvic-hip complex become vitally important in maintaining functionality. Muscle energy techniques and exercise regimes have been employed to maintain correct alignment and synergies. Further reading can be found elsewhere on this site : https://www.back-in-business-physiotherapy.com/we-do/muscle-energy-techniques.html
In the clinical scenario, the influence of physical, hormonal and emotional changes need to be taken into consideration if dealing with musculoskeletal dysfunction and exercise prescription. Specific interventions pertaining to assessment and treatment techniques can be found here : https://www.back-in-business-physiotherapy.com/we-treat/pregnancy-back-pain.html
Hormonal changes, specifically those which increase ligamentous laxity can not only change the dynamics of the pelvis, but may affect foot pronation, knee angles (knock knee) and the thoracic rings, even the neck. Moreover, pre-existing conditions may be amplified during pregnancy.
Elite athletes quite often need to time their pregnancy on world championship and Olympic cycles. They may also feel pressured to return to sport prematurely, both at a physical and psychological level. The prescribing physiotherapist needs to perhaps considered techniques in CBT and NLP when designing exercise programs. However, they may also need to show high levels of moral and ethical standards when dealing with athletes coaches, sponsors and managers, if the time isn't right to return to sport. Please see elsewhere, using post knee trauma as an example : http://cdnback-in-business-physiotherapy.r.worldssl.net/images/pdf/RTS_ACL_consensus_2020.pdf
There is a lack of evidence available to develop best-practice guidelines for the care of pregnant and postpartum elite athletes and women employed in arduous occupations. Hereby, the support needed, is given through experienced professionals, such as musculoskeletal sports physiotherapists, rather than guidelines. Each case needs to be treated individually by dividing people with 'complications' vs 'no complications'. Medical-Psychological-Musculoskeletal status should be established by considering, the type, scope and extent of activity wanting to be achieved and more importantly, the realistic timeframes and feedback mechanisms to be used to ascertain such a status. Good communication amongst a team of multidisciplinary specialists must ensue for optimal outcomes to be achieved (Jackson T et al 2022 Ex Sp Sc Reviews, 50, 1, 14-24). In this model, different specialists are required at different stages of the athletes journey, as a mother and as a returning 'super human'. During pregnancy, later as lactating breast feeding women and finally as an athlete, the importance of the nutritionist, will also need to be integrated into the process.
Currently, a pro-active approach to pregnancy and arduous activity only occur if pain or other medical complications occur. This is ingenuous to these very special women. A system of care should be established, involving situational specific functional criteria, as well as that of routine maternal care. Musculoskeletal assessments should probably be performed on, at least, a temporal trimester basis. Athletes themselves, should assess their appetite for sport participation risk through Psychometrics such as the Canadian Society of Exercise Physiology "Get Active Questionnaire for Pregnancy". Contrary to popular belief, complications associated with pregnancy such as low back pain and urinary incontinence can be prevented, or at least, not left until post partum to be treated.
In arduous occupations the duration of standing and walking should be restricted to 4 hours and the weight lifted to under 100kg (Cai C et al 2020 Am J Obst Gyn, 222, 3, 224-38). This does not consider the persons individual needs and shows an obvious deficiency in the guidelines.
Post partum, the uncomplicated pregnancy, can go through the three phases of individualised rehabilitation, as espoused by Bo et al (2017, Br J Sp Med,51, 21, 1516-25) and updated by Deering et al (2020J Orthop Sp Phys Ther, 50, 6, 281-4), whereby active recovery is followed by training and performance. The first phase deals with being a mother and health-birth related concerns. The training phase emphasises functional sports specific exercise, whilst the final phase of 'performance' relates to athletic abilities all the way to the competitive and recovery cycles of sport. This phase encompasses endurance training, periodisation, heart rate variability, psychological stages of injury and recovery, as well as immune considerations and can be read elsewhere on this site : https://www.back-in-business-physiotherapy.com/endurance-training.html . Importantly, these considerations shouldn't be restricted to elite athletes but also considered in women with arduous occupations.
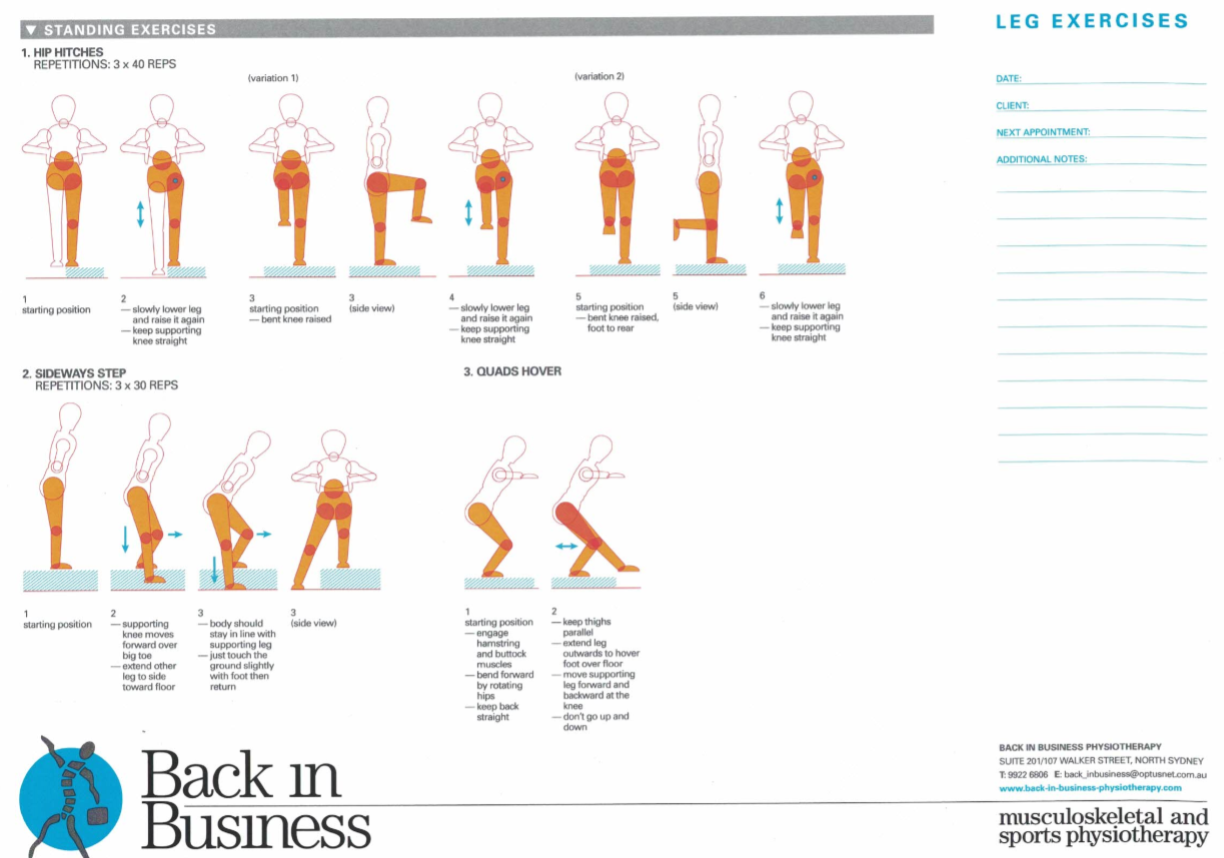
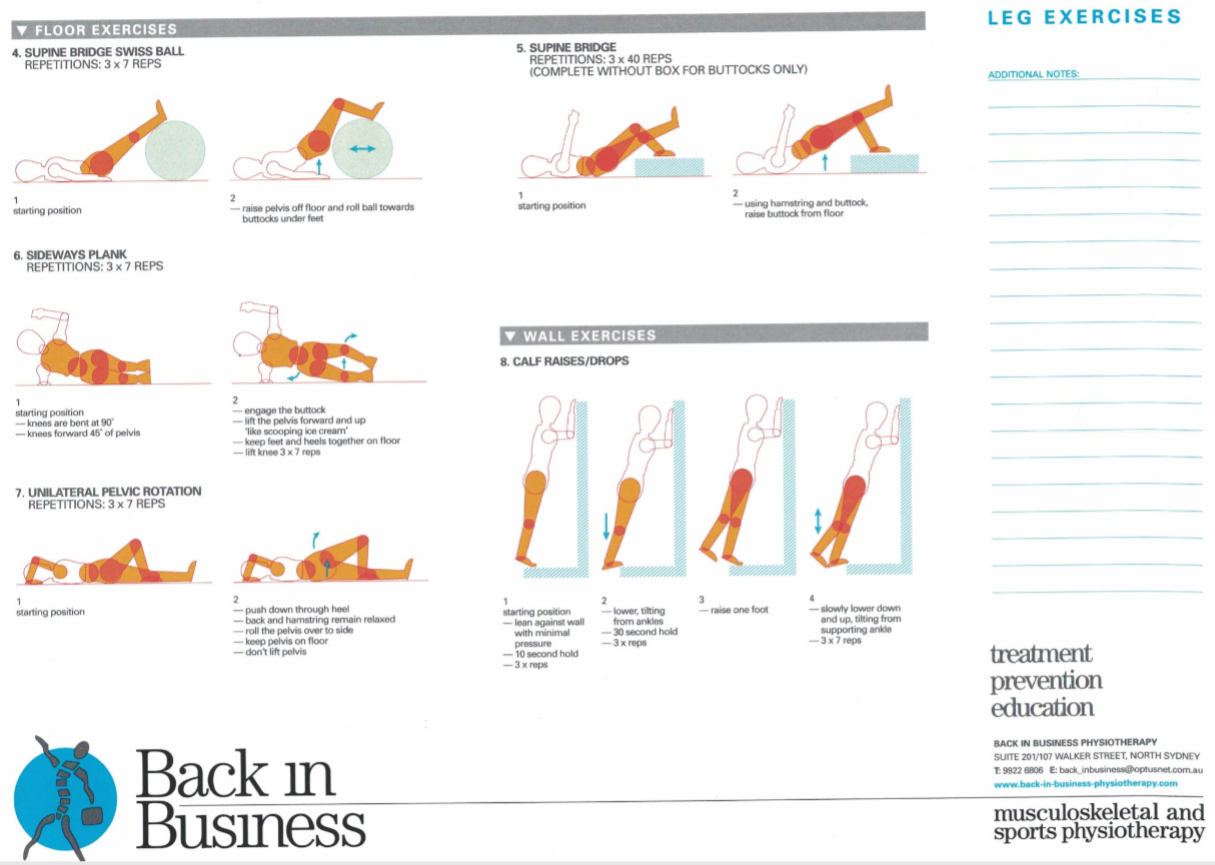
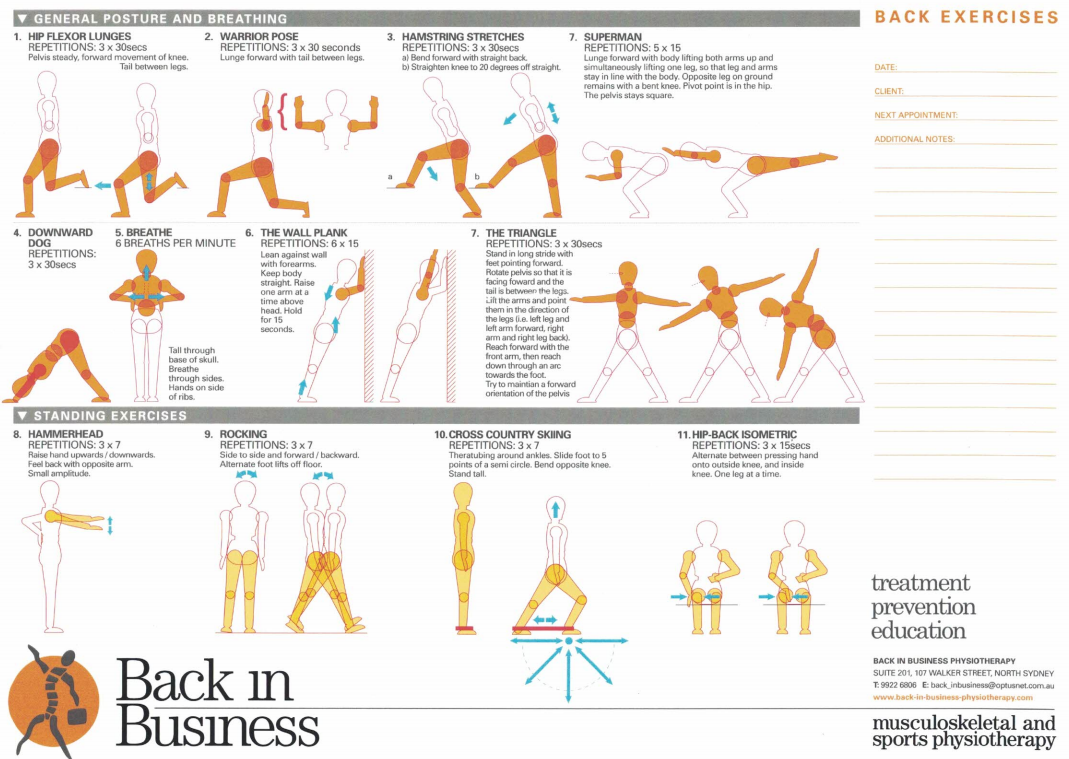
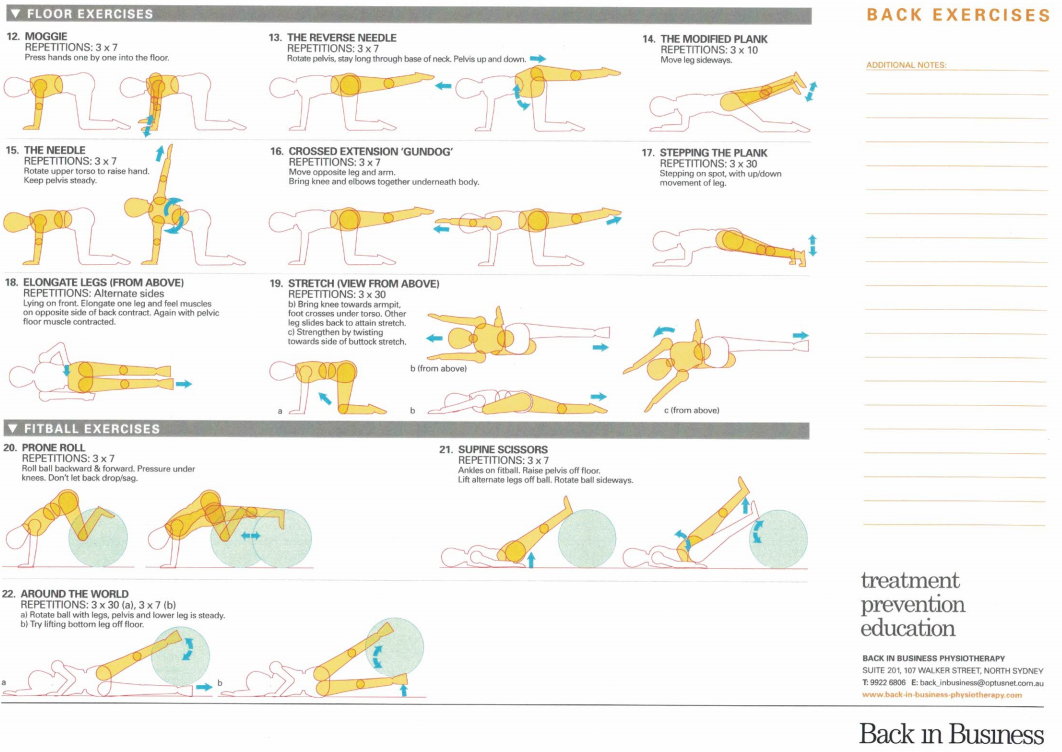
Crucially, in an athlete such as Alex Morgan, where pelvic and hip dynamics play such an important role to pregnancy itself, as well as to the integrity of the musculoskeletal system around the knee and back, truly functional exercises need to be integrated into the training program, which are appropriate for the stage of pregnancy and later the recovery and build up into the competitive season. Core stability and lumbopelvic - knee exercises are a critical part of this process.
Uploaded : 26 February 2022
Updated : 27 October 2022
